Why great medtech fails, even when it works
5 real examples showing why the value triangle determines what gets adopted.
Featuring insights from Ben Wright, co-founder of Mimetic MedTech Foundry, alongside founders building in the space: ShanShan Wang (Roam Tech AI), Dr Anushi Rajapaksa (Misti), Dr Dharmica Mistry (BCAL Diagnostics), and Dr Maryam Parviz (SDIP Innovations).
Understanding the triangle of value in Medtech is instrumental in creating value accross the healthcare system and drive adoption.
Why great medtech fails, even when it works
Everyone thinks medtech is a science problem.
It’s not, at least not solely.
You can have a breakthrough device, better outcomes, elegant engineering, years of research… and still never reach a single patient.
Because in medtech, success is not decided by the success of the tech itself.
It’s decided by a system, and a rather complex one.
1. The illusion: “If it works, it will win”
There is a belief in science that the primary driver of success is the quality of the tech. If it works, it will win.
In medtech, that’s not how it plays out.
As Ben Wright puts it:
“Compelling technologies often fail, not because they don’t work… but because they don’t fit.”
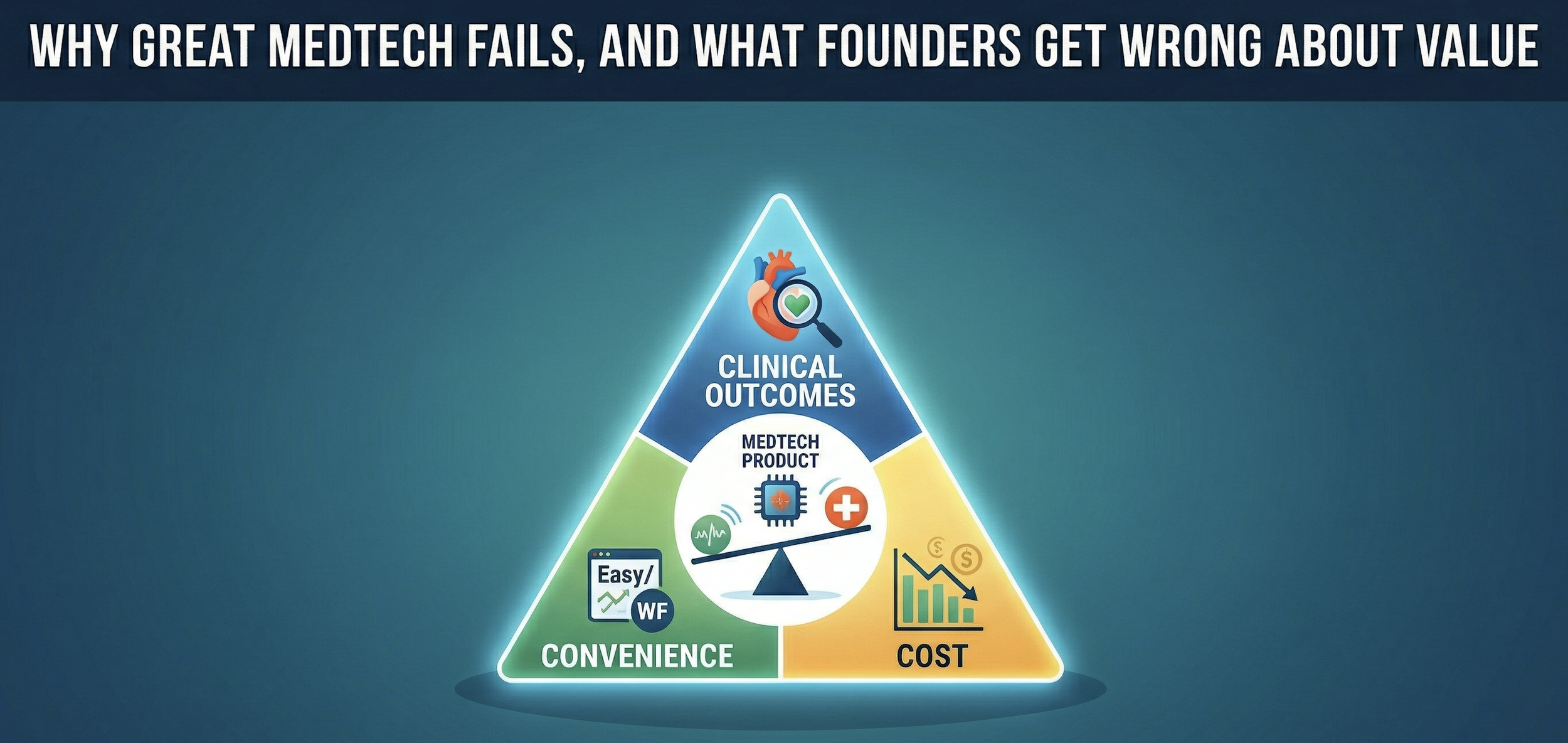
Value sits on a triangle:
✅ clinical outcomes
✅ convenience
✅ cost
You need to win on at least one. Ideally two.
But even that is not enough.
Because value is not one-dimensional.
It is negotiated across a system.
Same product. Different definitions of value.
Let’s look at an example: tankless portable oxygen, Juno, the product ShanShan Wang is developing at RoamTech AI.
Where does the value lie for each of the stakeholders?
From a patient perspective:
✅ lighter
✅ portable
✅ more freedom
Juno wins on convenience and quality of life.
From a clinician:
✅ reliability
✅ dynamic oxygen output
Juno wins on clinical outcome with the dynamic oxygen output, but will need to demonstrate the same reliability of the good old oxygen tank.
From a distributor:
✅ margin and business model
That’s where it gets tricky. Oxygen needs to be refilled, often.
❌ recurrent income would be wiped out with tankless oxygen pulling oxygen out of thin air
So the product will have to make commercial sense for the manufacturer and distributor.
Same product.
Three different expectations.
As ShanShan Wang explains:
“You have to be able to provide a value proposition for each of those stakeholders with just the one device. That’s the challenging part.”
If you optimise for one, you can break the others.
Often in medtech, the patient is not the customer.
In diagnostics, this becomes even more obvious.
A patient does not buy a diagnostic test.
The lab does.
Dr. Dharmica Mistry was developing a cancer blood test for breast cancer at a company she co-founded at age 22, while doing her PhD.
She explained:
“The customer at the end of the day is not the woman who has the test. It’s actually a pathology company.”
So your product needs to work for:
✅ the doctor
✅ the lab
✅ the system
✅ the workflow and at the scale and pace it needs to operate, not any slower
✅ the regulator
❌ Miss that… and no one can use what you built.
When you win on all three…
Some products do win across the triangle.
Dr. Maryam Parviz is developing a bioresorbable bone implant for surgery at SDIP Innovations, a company she co-founded as a university spin-off.
Their product, Jazbi, wins on all fronts:
✅ Better outcomes
No inflammation, no opening of another part of the body to get a bone graft, no second surgery for removal
✅ Better usability
It can be shaped on the spot and save surgeons 20–30 minutes on the surgery, and remove the need for a second surgery.
Time in theatre is gold, so that’s definitely a win.
✅ Lower cost
Like 30 times cheaper than the gold standard due to the material they use.
But here again, the patient isn’t the customer.
The clinician will be, and the payer is going to be insurer or Medicare, so with the promise of a cheaper and superior product bringing efficiencies in theatre and safety… in theory, we’ve got a winner, so watch this space.
When the system works against the patient
Take oral chemotherapy, specifically when “Xeloda” was launched in 1998 in the US.
It held the promise of chemotherapy at home, instead of lengthy clinic visits which can be hard for patients, especially in rural areas.
✅ Better for quality of life
✅ More convenient
And yet, it struggled to get adoption.
Fast forward to 2026.
There are a few challenges for Xeloda, including toxicity for patients with certain genetic profiles (i.e. with a dihydropyrimidine dehydrogenase (DPD) deficiency making it hard for the body to break it down) and poor tolerability leading to low compliance.
So this alone is enough to challenge adoption.
However, when it first launched and these toxicity issues and compliance were not obvious, another factor challenged the adoption of this oral chemotherapy.
The billing system disincentivised in 2 ways (1):
❌ Hospitals and clinicians had incentives to have patients come to the clinic due to hospital funding being linked to the nature and volume of medical services provided annually
❌ The payer (Medicare or insurer) would not pay the same amount for home therapy vs clinic therapy, thereby shifting more cost to the patient, which made it less accessible
As Ben Wright describes it:
“You’re disincentivising the physician to prescribe it… and shifting the cost to the patient.”
Better for the patient.
Worse for the system.
And the system won, at least for a bit.
The good news is that this view is shifting and over 25% of anticancer drugs under development are planned to be available as an oral formulation.
2. The team is not optional. It’s survival.
But even when the triangle of value is fulfilled and the tech fits nicely in the system, developing medtech has many more hurdles, including the team, what it can execute, and the funds it can raise.
Success depends on capital and timing.
Dr. Maryam Parviz explained how she prioritised her development plan to align with the next tranche of funding:
“Without capital, even if you have the best technology… you need to think about the next funding before this one finishes and focus on what will get you this next tranche of funding.”
And that brings us back to the team who can both deliver the strategy and raise the funds for it.
Often, the CEO plays an instrumental role in both building the team and bringing funding.
Speaking with Dr. Dharmica Mistry and Ben Wright, who both have long experience in helping medtech founders beside their own medtech experience, they both emphasise that no one builds medtech alone.
“Building medical device companies requires a village. No one can do it by themselves.” — Ben Wright
Strong founders build around their gaps.
The best founders don’t try to do everything. They build around what they don’t know.
As Dr. Anushi Rajapaksa puts it:
“If you do not have that expertise, then bring them in… and align them on the mission.”
And just as important:
“When you pick these people, you’ll be working with them for a long time. Trust and commitment need to be there.” — Dharmica Mistry
Dharmica's advice was simple:
✅ pick wisely
✅ define clear roles and responsibility
✅ ensure each contribution is rewarded fairly
Building a team is key, but having the right CEO in place is one of the most important leverage points.
The expensive dream of the scientist-CEO
We love the story of the scientist turned CEO.
The lab scientist making a breakthrough discovery, spinning off a company, and becoming the CEO, building a team and leading them through the whole adventure.
That’s a great story to tell.
But it’s not the most efficient path.
Let’s look at the bright side first:
It’s a story that can work.
There are plenty of commercialisation courses, incubators, accelerators, and mentoring programs to help scientists step up into the CEO role.
Most of the medtech founders I interviewed are following this path and we’re yet to see if they will hit patient adoption.
But certainly, these are extremely resourceful people, with extraordinary learning capabilities and storytelling skills to rally people and funding behind them.
Examples:
Dr. Maryam Parviz built a world-class team backed by serial medtech founders by accessing a prestigious world class incubator in San Francisco.
ShanShan Wang rallied investors after being triggered by seeing a child with an oxygen cylinder on a swing.
She has got a way of getting to people’s motivation to bring them on her team:
“If you have got such a short amount of time, don’t you want to make an impact? And if you see an issue affecting lots of people, and your skillset can solve it, why wouldn’t you do it” — ShanShan Wang
She is the CEO but partnered with a business-oriented co-founder.
Win-win.
And if we look at companies whith scientist CEO, there are enough examples to show it is possible.
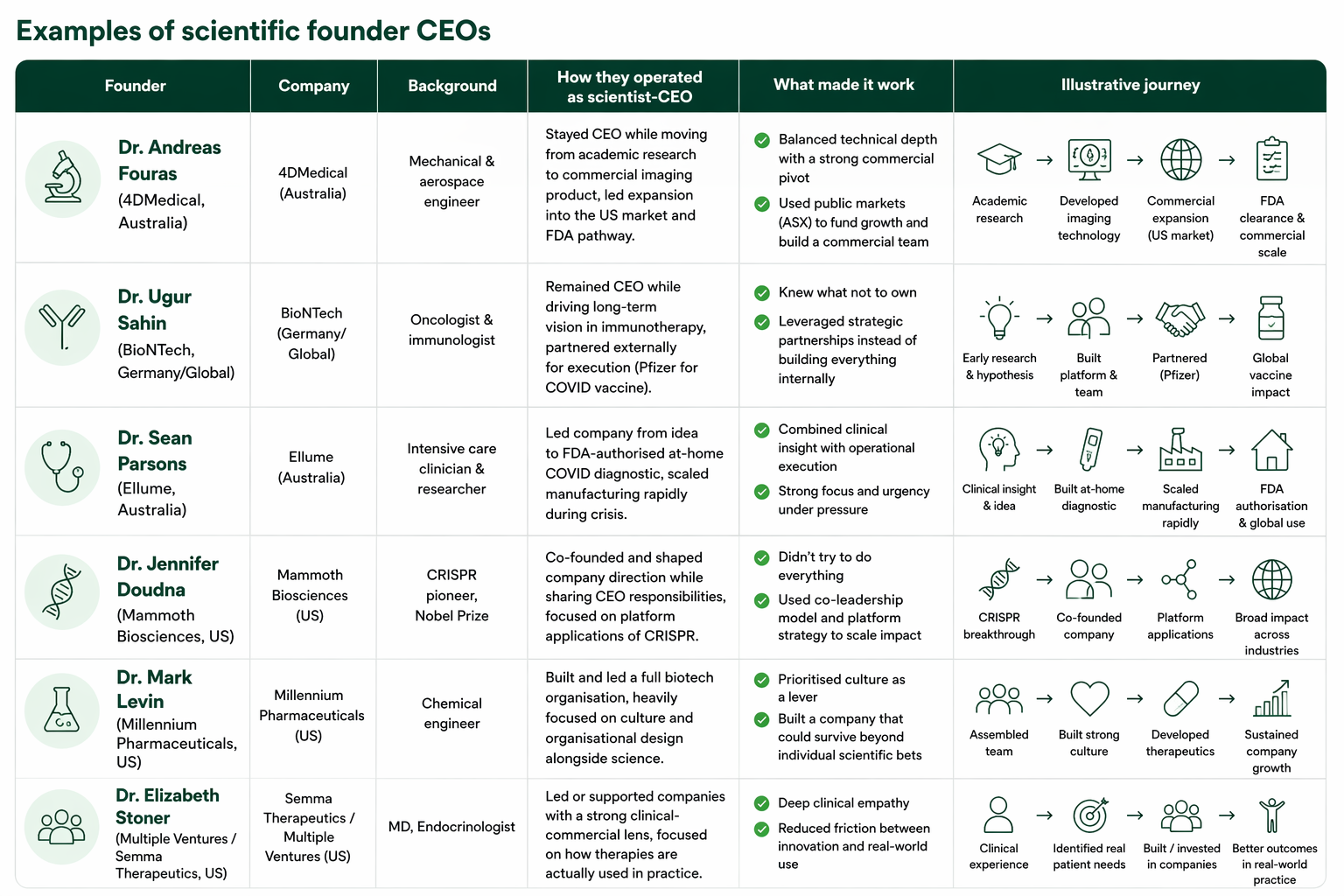
Examples of Scientific founder CEO of company with medtech on the market.
Possible. But it’s not the most efficient path.
As Dr. Dharmica Mistry, medtech co-founder and medtech commercialisation specialist at MTP Connect:
“Traditional scientific training doesn’t automatically translate to commercialisation training. They’re two very different worlds.”
These super scientists exist but as Ben Wright points out:
The scientists who:
a) want to do it (yes, embrace some of the boring stuff too)
b) are capable of doing it
These, they are a rare breed.
And not just that, for many scientists and clinicians, learning business on the job is possible but it has trade-offs:
❌ takes time
❌ costs money
❌ increases risk
It’s expensive, it is slow and it takes trial and error.
In short, it is not the most efficient path.
This is why venture studios, like Mimetic Studio, exist.
They bring:
✅ fractional leadership
✅ investment
✅ network
✅ execution
The expertise and the ecosystem to accelerate the company at these early critical stages.
They have skin in the game, so they are invested, quite literally, in your success.
As Ben Wright explains:
“Instead of a very smart academic and a very smart clinician working together with no business experience, they now have a business team with a clinical champion and a technical capability with a clear understanding of how they’re going to de-risk that product and take it to market. That’s a much more compelling investment proposition than when you’re approaching family offices and corporate venture capital.”
So if you’re the scientist who wants to become the CEO and you can do it without burning all your investor cash, Go you!
But there are alternatives.
And that’s a good thing.
If you want to hear more stories of the scientists CEO, Follow Multiple Hats.
3. Vision and storytelling is not optional
You can have the best technology in the room.
If people don’t understand it, it doesn’t matter.
As Ben Wright says:
“Scientists who can tell stories better… are more successful in getting grants.”
Your job is not to explain everything.
It’s to make people care.
As ShanShan Wang puts it bluntly:
“Your job is to make them care. And if you don’t say anything… how are they going to know?”
Practice makes perfect.
One of my favourite quote from Dr. Dharmica Mistry “ You gotta kiss a lot of frogs! It is not about getting it perfect but it is about understanding “Does my idea resonate? Is that person grasping what I'm trying to say? Do they understand the value of what I'm trying to achieve? And are they, you know, willing to come on this journey with me?”
Repetition is part of the job.
You don’t say it once.
You say it again and again.
“Increase your surface exposure until the stars align.” — ShanShan Wang
Final thought
If you’re building in medtech:
Know your triangle.
Build your team early.
And learn to tell your story.
Because the market doesn’t reward great science alone.
It rewards the people who can make others believe in it.
If you’re building in this space:
Be honest.
Are you solving for the patient…
or for the system that decides what gets used?
Because that’s where most good ideas fail.
Live episodes
In the conversation with Ben Wright, the idea is clear:
Good science is not enough.
What matters is whether something fits the system.
In my solo episode, I unpack how this actually plays out across 5 real examples:
• a portable oxygen device that makes sense for patients, but challenges existing care models
• a respiratory relief product that is easy to use, but struggles with positioning
• a cancer diagnostic navigating clinical pathways and adoption
• a bioresorbable implant balancing innovation with surgical practice
• and others navigating the same tension
Different products.
Different founders.
Same pattern.
If you optimise for one dimension,
you can break the others.
Listen to both perspectives
If you want to go deeper:
→ Start with the investor lens (Ben Wright) 🔗 listen here.
→ Then explore the real-world examples and real stories of medtech 🔗 listen here.
And if you want more medtech stories, Follow Multiple Hats
s